Technology has been the driver in the last 40 years of medical transcription changes. In fact, technology has been the driver since the beginning – but some have noticed that lately, it’s driving us to the wrong destination. The last 15 years or so have been particularly frustrating for physicians and clinicians. They would agree that “technology is a disruptor,” but not in the good way that EMR companies, voice recognition companies, and so many others in the tech sector want you to believe.
Here then is an overview of the 40 years of medical transcription changes, both good and bad.
Table of Contents:
- A Short History of Patient Records
- Technology Shifts Get Faster and Faster
- What the Software Engineers Forgot
- Voice Recognition Not Much to Write Home About
- Shifting Back to a More Human Approach
A Short History of Patient Records – 40 Years of Medical Transcription Changes
As mentioned above, the history of patient records goes back much further than just 40 years of medical transcription changes. The first known “written patient record” dates back to Egypt in 1,600 B.C. These papyrus strips contain detailed treatment instructions for war wounds.
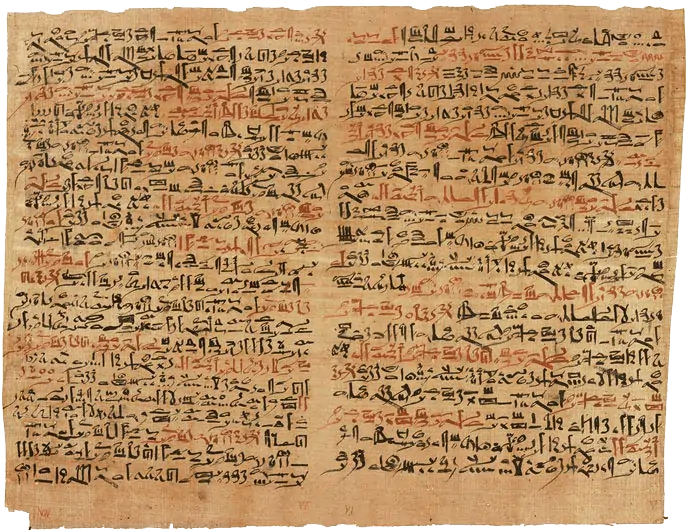
It’s hard to overestimate the huge impact this new technology – papyrus – had on medicine. For the first time, here was a portable document that could be replicated, read, and referred to giving best practices and medical tips. Today, we’re used to books and tweets and other written information in our daily lives. But doctors in Ancient Egypt must have felt on the cutting edge.
A thousand years later, Hippocrates started to write case histories of patients. The concept and practice were developed further in Roman Europe and the Middle East. But it wasn’t until 1752 that the first official system of patient records we know today was developed in Sweden. It provided a single, centralized repository of the patient’s disease, injury, and treatment history so that multiple clinicians could refer to and update the record.
Transcriptionists entered history somewhere near the beginning of the 20th century. Hospitals and other institutions found that it was vitally important to have a standardized way of recording patient histories. Medical stenographers would record notes by hand during rounds. Not only did these clerical professionals ensure the notes were recorded properly, it freed up clinicians to interact with their patients more closely. Obviously, that was a good thing!
Technology Shifts Get Faster and Faster – 40 Years of Medical Transcription Changes
In the 1980s, things really started to move – the beginning of our 40 years of medical transcription changes. At that point, probably the most advanced “technology” we were using was the microcassette. We’d receive them by bonded courier and return typed pages by the same. Doctors and clinics could slide these transcripts into the paper-based patient record. Easy peasy!
Telephone dictation started to get popular around this time. Of course, the word processor replaced the typewriter in a very short span – though we still printed them out in the beginning to send them back to the client. These were major shifts of course, but the way we did transcription was fundamentally the same.

That all changed with the rise of the electronic medical record or EMR (also called an electronic health record or EHR). This might not have had such a big impact on transcriptionists except for a curious marketing ploy – they were sold with the promise that it would “eliminate transcription.” Suddenly health networks, clinics, and small offices thought they’d found a way to save money.
Of course, companies can’t be faulted for being concerned about their bottom lines. But what nobody told them was that there would be a dark consequence to eliminating this clerical help. The biggest shift in 40 years of medical transcription changes turned out to be the fact that doctors would suddenly being doing the documentation work themselves.
What the Software Engineers Forgot: Transcription Saves Physicians Time and Money – 40 Years of Medical Transcription Changes
At the beginning of this post, we mentioned that technology doesn’t always drive us in the right direction. The rise of the EMR is a perfect example. To be clear, the EMR itself is a great innovation. Nobody is arguing how useful it is to have that patient data centralized like a paper record, but with much easier portability. Authorized health care workers can access those records from literally anywhere with an Internet connection.

But what the software engineers forgot – or at least downplayed – was that someone still has to input that data into the medical record. Eliminate transcriptionists, and you’re eliminating that valuable clerical help that hospitals at the beginning of the 20th century knew was so vital. Physicians and clinicians were thrust into the role of data processors. That’s the wrong approach on so many levels:
- Clinicians aren’t necessarily trained at data entry
- Physicians spend more time with their patient records than actually talking with patients
- Clinician burnout is on the rise due to the extra burden – and hours – of updating patient records
- Physicians and clinicians might see fewer patients as a result, reducing billables and losing income
- Physicians and clinicians repeatedly voice their frustrations with EMR systems
So these six-figure professionals are being asked to sacrifice their valuable time to do clerical work they once had help with. That approach doesn’t make sense on any level.
Voice Recognition Not Much to Write Home About – 40 Years of Medical Transcription Changes
Similarly, another big disruptor in 40 years of medical transcription changes that’s causing more problems than it’s worth is voice recognition. We all imagine a magical program that quickly and perfectly translates our speech to useable text. But here too, not all is as advertised. One medical transcriptionist summed it up nicely:
“Do you know how many he/she, left/right, misunderstood drugs and dosages that I have to correct in a day? Does voice recognition know the ins and outs of the physicians like I do? Does voice recognition have the ability to realize when things just do not make sense? No. It cannot do any of these things.”
So, even assuming that VR software works with 100% efficiency (which is does not – not even close), there will still be errors that only an experienced transcriptionist could pick out. The result: physicians and/or office staff are left reviewing and correcting – and correcting and correcting – page after page of VR transcription. If it takes longer to fix than to do properly in the first place, is it really saving you time and/or money? It’s the same empty electronic promises: sounds perfect in theory, but the reality in the field is a lot messier.
Shifting Back to a More Human Approach – 40 Years of Medical Transcription Changes
At iMedat, we’re suggesting we shift back a little bit on those 40 years of medical transcription changes to a time when physicians and clinicians had the help they need. Yes, let’s use and embrace EMR technology. But let’s use it properly, as we would any tool. That means:
- Instead of asking clinicians to update their own patient records, get documentation experts do it for them
- Instead of putting physicians’ attention on a computer screen, we put it back on their patients where it belongs
- Instead of forcing physicians and clinicians to see fewer patients, we take as much off their plates as possible so that they can see more patients, boosting billables – and patient satisfaction

iMedat provides customized medical transcription services for doctors and clinicians so that they can get fast, easy clerical help. And when we say customized, we mean customized – right down to the individual clinician. Everyone has their own way of doing things. So, if Doctor A personally likes using the EMR for some things but wants to dictate others, we can handle that. If Specialist B wants to dictate everything and focus more on the patient, we can handle that too.
We know too that it’s not all about EMR for everyone. We support offices that still prefer to use paper-based patient records, tailoring a transcription solution that works best for your office.
Contact iMedat to learn how our professional medical transcriptionists can help improve your office workflows and make patient care more human again.